
What is lichen sclerosus?
Lichen sclerosus is common chronic skin disorder that most often affects genitalia and perianal zones
Old names for lichen sclerosus (LS) include lichen sclerosus and atrophicus, vulvar kraurosis (in women), and balanitis xerotica obliterans (in males).
Who gets lichen sclerosus?
Lichen sclerosus can start at any age, although it is most often diagnosed in women over the age of 50. Prepubertal children can also be affected.
- Lichen sclerosus is ten times more common in women than in men.
- The 15% of patients know a relative with lichen sclerosus.
- May follow or coexist with another skin condition, most commonly lichen simplex, psoriasis, erosive lichen planus, vitiligo or morpho.
- People with lichen sclerosus often have a personal or family history of someone else. autoimmune disease such as thyroid disease (approximately 20% of patients), pernicious anemiaor alopecia areata.
What Causes Lichen Sclerosus?
The cause of lichen sclerosus is not fully understood and may include genetichormonal irritating, traumatic and infectious components.
Lichen sclerosus is often classified as an autoimmune disease. Autoimmune diseases are associated with antibodies to a specific protein.
- The extracellular matrix Antibodies to protein 1 (ECM-1) have been detected in 60 to 80% of women with vulvar lichen sclerosus.
- Antibodies against other unknown proteins can explain other cases, which explains the different presentations of lichen sclerosus and the response to treatment.
- However, these antibodies could be epigenetics, that is, the results of the disease rather than the cause of the disease.
Male genital lichen sclerosus is rare in men who are circumcised in childhood. It has been suggested that it may be caused by chronic and intermittent urine damage occluded under the foreskin
Since the onset in women is commonly postmenopausal, a relative lack of estrogen can be significant
What are the clinical features of lichen sclerosus?
Lichen sclerosus appears as white patches of wrinkled or thickened skin that tend to scar.
Vulval lichen sclerosus
Lichen sclerosus mainly involves nonhair bearing, internal areas of vulva.
- Can be located to a small area or involve widely perineum, labia minora (inner labia) and hood of the clitoris.
- It can spread to the surrounding skin of the labia majora and inguinal fold and, in the 50% of women, to the anal and perianal skin.
- Lichen sclerosus never involves vagina mucous membrane.
Lichen sclerosus can cause extreme itching and pain (pruritus vulvas)
- Sometimes bruises, blood blisters and ulcers appear after scratching, or from minimal friction (eg, tight clothing, sitting).
- Urine can itch and irritate.
- Sex can be very uncomfortable and painful. fissure of the later Fourchette at the entrance to the vagina.
- It can cause discomfort or bleeding when passing stools and aggravate any tendency to constipation, especially in children.
Lichen sclerosus causes adhesions and scars.
- The clitoris may be buried (phimosis).
- The labia minora are reabsorbed / shrunk.
- The entrance to the vagina becomes tight (introital stenosis)
See more images of lichen sclerosus vulvae.
See more images of perianal lichen sclerosus.
Lichen sclerosus of the penis
In men, lichen sclerosus usually affects the tip of the penis (glans), which becomes white, firm, and scarred.
- The urethra can narrow (meatus stenosis), resulting in a thin or crooked urinary flow.
- The foreskin can become difficult to retract (phimosis).
- Sexual function can be affected due to painful erections or embarrassment.
See more pictures of lichen sclerosus of the penis.
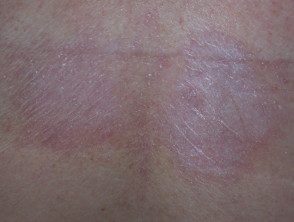
Extragenital lichen sclerosus
Extragenital lichen sclerosus refers to lichen sclerosus at other sites.
- Extragenital lichen sclerosus affects the 10% of women with vulvar disease.
- Only 6% of men and women with extragenital lichen sclerosus do not have genital lichen sclerosus at the time of diagnosis.
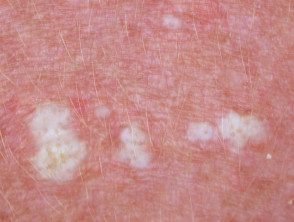
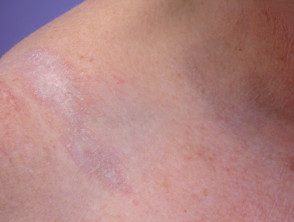
One or more dry whites plates It can be found on the inner thigh, buttocks, lower back, abdomen, under the breasts, neck, shoulders, and armpits.
- Lichen sclerosus looks like cigarette paper in that the skin is dry, wrinkled, and thin (atrophic)
- Hair follicles may appear prominent, containing dry plugs of curb.
- Bruises, blisters and ulcers may appear without being noticed trauma.
Nongenital lichen sclerosus

Lichen sclerosus
Lichen sclerosus
Lichen sclerosus
Lichen sclerosus

Lichen sclerosus

Lichen sclerosus
See more pictures of extragenital lichen sclerosus.
What are the complications of lichen sclerosus?
Infections
Patients with lichen sclerosus can develop infections, particularly Candida albicans, Herpes Simplex, Staphylococcus aureus. Herpes infections are particularly painful and can cause vulva ulceration.
Scaly cell carcinoma
Lichen sclerosus from anogenital sites are associated with increased risk of vulva, penis, or anal Cancer (squamous cell carcinoma, SCC).
- Cancer is estimated to affect up to 5% in patients with vulvar lichen sclerosus.
- Cancer is more likely if the inflammatory The disease is not controlled.
- Invader SCC appears as an enlarged lump or a sore that will not heal.
-
High-grade squamous intraepithelial lesions in women (SIL) or men associated with lichen sclerosus may be associated with HPV (usual type) or differentiated.
Extragenital lichen sclerosus does not appear predispose cancer
How is lichen sclerosus diagnosed?
An experienced doctor can often diagnose lichen sclerosus by its appearance. Skin biopsy It is frequently recommended.
- Histopathology can confirm the suspected diagnosis of lichen sclerosus.
- Another skin condition can be diagnosed or coexist with lichen sclerosus.
- A focal The area may be biopsied to evaluate for cancer or SIL.
A biopsy may also be recommended at follow-up, to assess areas of concern or to explain inadequate response to treatment.
What is the treatment for lichen sclerosus?
Lichen sclerosus patients are best to consult a physician with a particular interest in the condition for an accurate diagnosis and treatment recommendations.
It is advised that you become familiar with the location and appearance of your lichen sclerosus.
- Women can use a mirror when applying current therapy.
- Photographs can help monitor activity and treatment.
General measures for genital lichen sclerosus
- Gently wash once or twice a day.
- Use a soap-free cleanser, if there is one.
- Try to avoid tight clothing, rubbing, and scratching.
- Activities such as riding a bicycle or horseback can aggravate symptoms.
- If you are incontinent, seek medical advice and treatment.
- Apply emollients to relieve dryness and itching, and as a barrier to protect sensitive skin in the genital and anal areas from contact with urine and feces.
Topical steroid ointment
Topical steroids are the primary treatment for lichen sclerosus. An ultra-potent topical steroid is often prescribed, for example, clobetasol propionate 0.05%. A potent topical steroid, for example, mometasone furoate 0.1% ointment, can also be used for mild illness or when symptoms are controlled.
- An ointment base is less likely to cream sting or cause contact dermatitis.
- A fine stain should be applied to the white plates and rubbed gently.
- Most patients will be instructed to apply the steroid ointment once a day. After one to three months (depending on the severity of the disease), the ointment can be used less often.
- It may be necessary to continue topical steroids once or twice a week to control symptoms or to prevent lichen sclerosus from recurring.
- The itching often goes away within a few days, but it can take weeks or months for the skin to return to normal (if it does).
- A 30g tube of topical steroid should last 3-6 months or longer.
The doctor should reevaluate the treated area after a few weeks, as the response to treatment is quite variable.
Topical steroids are safe when used properly. However, overuse or over-application on the wrong site can lead to adverse effects. In anogenital areas, these include:
- Red and thin skin
- Burning discomfort
- Periorificial dermatitis
- Candida albicans infection (e.g vulvovaginal thrush)
It is very important to follow the instructions carefully and to attend your follow-up appointments regularly.
Other topical therapy
Other topical treatments used in patients with lichen sclerosus include:
- Pessaries or intravaginal estrogen cream in postmenopausal women. These reduce symptoms due to atrophic vulvovaginitis (dry, thin, cracked and vulvar and vaginal sensitive tissues due to hormonal deficiency).
- Topical calcineurin inhibitors, tacrolimus ointment, and pimecrolimus cream instead of or in addition to topical steroids. They tend to cause burning discomfort (at least for the first few days). Early concern that these drugs may have the potential to accelerate cancer growth in the presence of oncogenic The human papillomavirus (the cause of genital warts) seems unfounded.
-
Current retinoid (eg, tretinoin cream) is not well tolerated on genital skin, but can be applied to other sites affected by lichen sclerosus. Is reduced climbing and dryness
Oral medications
When lichen sclerosus is severe, acute, and does not respond to topical therapy, systemic treatment can rarely be prescribed. Options include:
-
Intralesional or systemic corticosteroids
- Oral retinoids: acitretin, isotretinoin
- Methotrexate
- Cyclosporine
Surgery
Surgery is essential for high-grade squamous intraepithelial lesions or cancer.
In males circumcision It is effective in lichen sclerosus that affects the foreskin and glans of the penis. It is best to do it early if the initial topical steroids have not controlled the symptoms and signs. If the urethra is tight or scarred, reconstructive surgery may be necessary.
In women, the release of vulvar and vaginal adhesions and the healing of vulvar lichen sclerosus may occasionally be done to reduce urination difficulties and allow intercourse if dilators have not been shown to be effective. The procedures include:
- Simple perineotomy (a division of adhesions)
- Fenton procedure (a incision that is repaired transversely)
- Perineoplastyexcision of affected and vaginal tissue mucous membrane Advance)
Unfortunately, lichen sclerosus sometimes closes the vaginal opening again after surgery initially seems successful. Can be repeated
Other treatments
Other reported treatments for lichen sclerosus are considered experimental at this time.
- CO2To be ablation of hyperkeratotic plates
-
Er: YAG laser
- Phototherapy
- Photodynamic therapy
- Fat injections
- Stem cells and platelet-Rich plasma injections
What is the prognosis for lichen sclerosus?
Lichen sclerosus is a chronic disease and generally persists for years.
- Extragenital lichen sclerosus is more likely to go away than genital disease.
- Early treatment occasionally leads to long-term, full treatment. remission.
- The scarring is permanent.
Long-term follow-up is recommended to monitor the disease, optimize treatment, and ensure early cancer diagnosis.