
What is Sjögren? syndrome?
Sjögren's syndrome (SS) is a autoimmune disease that mainly affects the secretory glands of the eyes and mouth, preventing them from producing tears and saliva properly (symptoms of sicca). SS produces dry eyes (called keratoconjunctivitis sicca), dry mouth (xerostomia), and sometimes arthritis. It develops slowly. When tested, most people with the condition have a positive blood test for anti-Ro antibodies.
Many SS patients have some characteristics of other autoimmune diseases, such as systemic sclerosis, systemic lupus erythematosus, or rheumatoid arthritis. In this case, they are said to have an overlap syndrome or SS is said to be secondary to the other autoimmune condition. The patient is said to have primary SS if other conditions are not present.
Who gets primary Sjögren's syndrome and how often does it develop?
Primary SS is 9 times more common in women than in men. It is especially common in older women. However, anyone can develop it. Up to 2% in older women has been found to have primary SS.
What is the cause of Sjögren's syndrome?
The cause of the SS is not known. One theory is that viruses (such as the Epstein-Barr virus) may play a role in activating SS in people whose genetic the fund predisposes them to SS. However, once the condition has been activated, there is a infiltrate of lymphocytes in the secretory glands. This is a slow and low degree inflammatory process that can cause damage to the gland cells and, therefore, impair the function of the glands.
Clinical characteristics of Sjögren's syndrome.
Eye problems in SS
Patients generally describe dry, sandy eyes. They may also feel burning discomfort, notice decreased tear production, increased eye fatigue, and sometimes intolerance to bright lights (photophobia) These symptoms can develop due to increased dryness of the eyes causing damage to the lining of the cornea in the front of the eyes.
Dry mouth
This can develop very gradually over several years. When first noticed, it can only be the feeling of dry mouth. As patients progress, they may notice difficulty swallowing dry food, difficulty speaking for long periods of time, problems with dentures, and sometimes increased tooth decay. Oral yeast infection is also more likely to develop.
Skin signs
The most common cutaneous manifestation is dry or rough skin (xerosis), which is observed by more than half of the patients. This can cause itching. SS patients also sweat less than people without the disease. Although these symptoms are common, most SS patients are more bothered by dry mouth and dry eyes. Vaginal dryness can also occur.
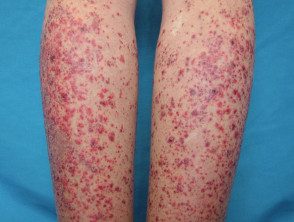
Vasculitis (inflammation of blood vessels) is potentially more serious. This develops in approximately 10% of patients with primary SS and affects the skin in half of them (cutaneous small vessel vasculitis). Skin lesions generally present as multiple purple or reddish brown spots. The color is due to bleeding from small inflamed vessels. Vasculitic skin lesions are more common and prominent on the legs, but can develop anywhere. They may present as flat red spots, raised bumps, blisters, ulcers or a high urticaria-I like it cure.
Other skin changes that have been reported in primary SS include:
- Cancel erythema (red ring-shaped patches) has been observed in Japanese patients
- Livedo reticularis
- Erythema nodosum
- Diffuse hair lost
- Vitiligo
- Raynaud's phenomenon
Sjogren's syndrome - cutaneous vasculitis
Sjogren's Vasculitis

Sjogren's Vasculitis

Sjogren's Vasculitis
Involvement of other organs in Sjögren's syndrome
Gastrointestinal system
Rarely, the gastrointestinal system can be affected in SS. The resulting dryness can inflame the lining of the esophagus (esophagitis) and the stomach (atrophic gastritis).
Light
Although SS can affect the lungs, it is rarely serious. The most common manifestation is a dry cough, due to dryness of the small airways.
Joints
Up to 60% of people with SS will eventually develop at least one episode of arthralgia (joint pain) or arthritis (inflammation within the joint). Arthritis generally does not produce erosion joint structures or joint deformity.
Kidneys
Kidney involvement is more common if SS is present as part of an overlap syndrome with systemic lupus erythematosus. It can affect the kidneys in several ways, including interstitial nephritis, kidney stones or glomerulonephritis.
Vasculitis
Primary SS vasculitis can damage the kidneys, lungs, nerves and joints. Fevers and anemia It may also be present. Involvement of the internal organs is more likely if vasculitis is associated with cryoglobulins (a special form of protein that precipitates at low temperatures). Some patients with primary SS and vasculitis have an underlying B cell. lymphoma (Cancer of the lymphatic system).
Long-term forecast Sjögren's syndrome
In long-term studies, reduced glandular function in SS has not been observed to improve. If arthritis, Raynaud's phenomenon, or interstitial nephritis are present early in the course of the disease, they can resolve with treatment and time. Worst forecast Factors include the presence of glomerulonephritis, decreased C4 blood levels complement, vasculitis and cryoglobulinemia.
Laboratory tests for Sjögren's syndrome
In people with symptoms that are consistent with SS, a variety of tests can be done to help confirm the diagnosis.
Schirmer test
This measures the wetting of a standardized tear strip applied between the eyeball and the side edge of lower eyelid. The test is considered positive if the result is less than 5 mm in 5 minutes.
Biopsy of salivary glands in the mouth.
A typical inflammatory cell infiltrate supports the diagnosis.
Anti-Ro and anti-La antibodies (blood tests).
In the correct clinical setting, the presence of these antibodies supports the diagnosis of SS.
Other tests that can be performed in special circumstances include measurement of salivary flow, parotid gland sialography and salivary scintigraphy.
Treatment of Sjögren's syndrome
The basis of treatment for dry eyes, dry mouth and dry skin is to minimize symptoms by replacing reduced secretions. There is no cure for the SS. Immunosuppressive medication is reserved for cases that have internal organ involvement and is most often used for severe kidney or lung disease.
Dry eyes
Artificial tears and ocular Lubricants are the most used. In severe cases, these may be necessary as often as every 30 minutes.
Dry mouth
The patient usually takes an increase in oral fluid as a method of trying to relieve symptoms. Other measures include the use of artificial saliva that can come in the form of gels, lozenges, or sprays. There is also a medicine called pilocarpine that can increase the secretion of damaged glands, although it does not cure the problem or reverse damage to the glands. Pilocarpine can be taken in tablets with each meal and at bedtime to increase saliva. Stop smoking, if applicable.
Dry Skin
Moisturizers and emollients It can be applied as needed. Choose a soap-free cleaner. A standard water-based lubricant can be used to relieve dryness of the vagina.
Arthritis
Nonsteroidal anti-inflammatory Drugs are the first-line medication for joint pain. Prednisone may be prescribed for severe illness or if symptoms do not improve with nonsteroidal treatment. Hydroxychloroquine has also been found to be helpful in some people.
Vasculitis
Systemic steroids (prednisone) and immunosuppressive medications such as azathioprine may be necessary.
Patients with SS should try to avoid medications with anticholinergic side effects (tricyclic antidepressants such as amitriptyline, antipsychotics, and antihistamines), as these can aggravate the symptoms of dryness.