

Ad
Skin cancer
Application to facilitate skin self-examination and early detection. read more.
What is it ocular melanoma?
Melanoma is a evil one tumor of melanocytes. Ocular melanoma refers to melanoma of the eye and represents approximately 5% of all melanomas [1]. Primary Ocular melanoma is the most common primary malignant tumor of the eye in adults [2].
Normal anatomy of the eye.
- Conjunctiva - the membrane in the external aspect of the eye.
- Sclerotic - the white of the eye, an opaque fibrous protective layer around the eye. It is continuous with the cornea.
- Cornea: the clear frontal surface of the eye.
- Iris: the colored part of the eye. May control The amount of light that enters the eye when opening and closing.
- Ciliary body: a muscle that allows the eye to focus by changing the shape of the lens.
- Choroid: A layer of tissue in the back of the eye between the sclera and the retina.
Melanocytes
Melanocytes are cells that produce pigment (melanin) Dark skin has more active melanocytes than light skin. Melanocytes produce more melanin in response to sun exposure and can produce patches pigmentation on the surface of the eye, called melanosis.
Melanocytic naevi
Melanocytes are often grouped as pigmented moles on the skin, properly called melanocytic nevi. They are harmless. Melanocytic nevi can also arise in the conjunctiva. Sometimes they are present at birth (congenital melanocytic nevus)
The collections of melanocytes in the deepest tissues of the eye are called ocular melanocytosis. Ota naevus is a form of dermal melanocytosis that can affect the eye.
What parts of the eye are affected by melanoma?
Primary ocular melanomas can be divided into 2 types:
- Uveal melanomas: arise within the iris, choroid and ciliary body. They are the most common form of ocular melanoma, with a stable report. incidence of 7 per million per year in the United States. Most cases (more than 90%) involve the choroid. Approximately 6% affects the ciliary body and 4% affects the iris.
- Conjunctival melanomas. They are less frequent although the incidence is increasing. Conjunctival melanomas have an incidence of less than 5 cases per million per year.
Uveal melanoma seen through slit lamp * (4 chiroid, 1 iris)

Uveal / choroidal melanoma

Uveal / choroidal melanoma

Uveal / choroidal melanoma
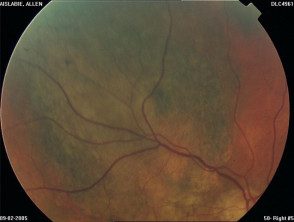
Uveal / choroidal melanoma
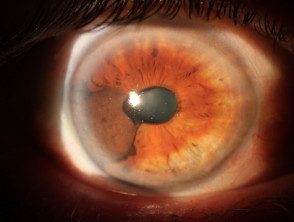
Uveal / iris melanoma
* Images provided by Dr. Stephen Guest
Cutaneous Melanoma can also affect the eyelid, but they are not considered ocular melanomas.
Melanoma affecting the eyelid **

Melanoma of the eyelid
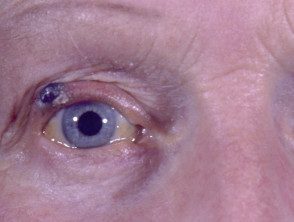
Melanoma of the eyelid
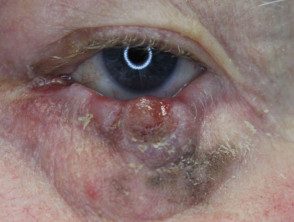
Melanoma of the eyelid

Melanoma of the eyelid

Melanoma of the eyelid
** Images provided by Dr. Stephen Ng
What is the cause of ocular melanoma?
Like other forms of melanoma, ocular melanoma occurs due to genetic changes within melanocytes that cause cells to proliferate. Other changes in the cells cause them to invade the surrounding tissues and spread to other parts of the body (metastasis)
Many reports suggest that exposure to sunlight may be an important factor in the development of ocular melanoma.
Who gets eye melanoma?
Both men and women appear to have the same incidence of ocular melanoma. The maximum incidence of presentation is closer to 62 years of age.
People at increased risk for ocular melanoma are Caucasian and have fair skin and light iris color. However, melanoma can also affect people with darker skin and eye color.
Melanosis, congenital ocular melanocytosis and neurofibromatosis They are also associated with increased risk.
Conjunctival melanoma patients tend to have many melanocytic (lunar) nevi. Approximately 20% is believed to arise from nevi and approximately 60-75% within conjunctival melanosis.
How is the diagnosis of ocular melanoma made?
The diagnosis of ocular melanoma is usually made by an accurate clinical examination. The main indicators of disease in 90 patients described in a Canadian study were: [3]
- Partial loss of visual field (in 33% patients)
- sun sensitivity (at 20%)
- blurred vision (at 20%)
- incidental finding on eye exam (at 17%)
Conjunctival melanoma presents as an increasingly irregular pigment injury in the external eye
Other symptoms may include a protruding eye, change in iris color, red or painful eyes, and retinal detachment.
Ocular melanoma progression.
Half of all patients develop metastatic disease within 15 years after treatment of the primary tumor. Unfortunately there is no cure for metastatic disease.
Metastasis It occurs by local spread or spread of blood. Transscleral spread can occur ciliary. nerves, veins, arteries or aqueous drainage channels. There is not lymphatic network in the uveal tract. Distal metastasis they occur in the liver in more than 80% cases. The lung, bones, and skin are also sometimes involved.
Poor forecast is associated with:
- large tumor size
- ciliary body involvement
- age of the elderly patient.
When treated early, iris melanoma is less likely to affect vision or metastasis compared to other uveal melanomas.
Histological Features associated with increased metastatic risk include:
- the presence of epithelioid cells morphology
- increased infiltration with immune cells
- tall mitotic Speed
- increased microvascular density
- loss of BRCA-associated protein 1 staining.
Chromosomal changes in ocular melanoma
Advances in detecting genetic changes in melanoma allow the diagnosis of tumors with high metastatic potential.
- BRAF mutations They are common in iris melanomas (such as cutaneous melanomas) but are extremely rare in other types of uveal melanoma.
- GNA11 or GNAQ mutations are found in the 80-85% of uveal melanomas and are early events in the development of non-cutaneous melanoma. The presence of these mutations are not forecast for posterior metastatic potential. GNAQ / GNA11 mutations are also seen in ocular melanocytosis, blue nevi, and Ota nevi. [4,5]
-
Mutations in BRCA1-associated protein 1 (BAP-1) and splicing factor 3B subunit 1 (SF3B1) occur later in disease progression. The presence of BAP-1 mutations is strongly associated with metastatic disease. A more favorable result is associated with the presence of SF3B1 mutations.
Genetic alterations associated with a worse prognosis in uveal melanoma include:
-
Inactivation of BRCA1-associated protein 1 (BAP1);
- Subsequent loss of a copy of chromosome 3 (Monosomy 3), which reduces survival to 5 years in a 50%;
- Additional gain of chromosome 8.
Gain of chromosome 6p is associated with a better prognosis and can act to delay or prevent the loss of chromosome 3.
What tests are performed on ocular melanoma?
The tests chosen depend on the clinical presentation and what is available. They may include:
- Eye fundus image / photography
- Ultrasound eye scan
- Biopsy tumor
- Connecticut eye and brain scan
- Liver ultrasound
- PET-CT scan.
What is the treatment for ocular melanoma?
Local treatments for ocular melanoma have improved, with greater preservation of normal ocular tissue, however, survival rates remain unchanged.
Uveal melanoma
License plate radiotherapy
- The radioactive seeds (most often iodine-125) contained within a small disc or plate are placed on the outer side of the eye that covers the tumor. After a few days the plate is removed.
Surgical resection
- Iridectomy
- Choroidectomy
- Enucleation (removal of the affected eye) if tumors thicker than 8 mm or orbital spread is extensive
Other
- Transpupillary phototherapy / thermotherapy: Infrared lasers heat the tumor a few degrees to interrupt cellular metabolism. This treatment is often used in conjunction with radiation therapy to reduce the incidence of local infections. reappearance.
- External proton beam radiation therapy can give high rates of local control, however, significant vision loss can also occur.
- Gamma knife stereotactic radiosurgery
Conjunctival melanoma
Conjunctival melanoma is treated by:
- spacious premises excisionand
- assistant therapy like brachytherapy cryotherapyor application of a current chemotherapeutic agent
Metastatic ocular melanoma
The prognosis in patients with metastatic disease remains poor. Options for metastatic melanoma of the eye may include:
- Chemotherapy using melphalan injected directly into liver metastases
- Surgical removal of the affected part of the liver.
-
Ipilumumab immunotherapy. Is monoclonal antibody blocks a antigen in cytotoxic T lymphocytes so that the immune system can attack melanoma cells.
- Internal selective radiotherapy, which involves the infusion of radioactive yttrium beads into the liver, where they accumulate within melanoma cells.
What happens in the follow-up of ocular melanoma?
After treatment of the primary tumor, regular follow-up is important to verify local recurrence or systemic spread.
Because the liver is the most common first site of systemic spread, it is often the subject of follow-up investigations, such as liver function tests, abdominal ultrasound, and abdomen. magnetic resonance image (Magnetic resonance)
What is the prognosis for patients with ocular melanoma?
Unfortunately, metastatic melanoma remains the leading cause of death among patients with ocular melanoma. The extent of systemic spread and tumor burden determines the average duration of survival after liver metastases have been detected.
