
What is it linear IgA bullous disease?
Linear IgA bullous disease is a autoimmune blistering disease in which blisters form on the skin and mucous membranes Its name comes from the characteristic findings in direct immunofluorescence of a skin biopsy, in which an IgA line antibodies can be found just below the epidermis. Also called linear IgA disease, and in children, chronic childhood bullous disease.
Who gets linear IgA bullous disease?
Linear IgA bullous disease affects adults of all ages, but is more common in old age. It's very weird. In some cases, it is associated with a medication.
Linear childhood bullous IgA skin disease It is also rare. It has been suggested that it may be more common in children in developing countries. It is more frequent in preschool children.
What are the clinical features of linear IgA bullous disease?
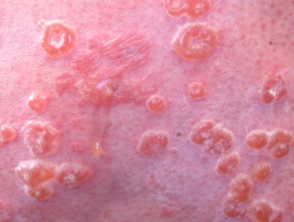
Linear IgA bullous disease is characterized by blisters on the skin and mucous membranes. They tend to start at the extremities, but any area of the body can be affected. Blisters and ulcers on the lips and inside the mouth it affects approximately 50% in people with linear IgA disease.
In boys, linear IgA bullous disease usually occurs before puberty with a sudden onset of blisters in the genital region, which then affects the hands, feet, face, and extremities.
Round or oval blisters filled with clear fluid may arise from normal-looking skin or from flat or raised red patches. Blisters may be small (vesicles) or big (bullas) Typically, the blisters are arranged in rings (cancel injuries) and can form an objective shape. The tendency for new blisters to appear on a ring around an old one is called a bead chain sign, and groups of small blisters can be described as a group of jewels. Secondary injuries include scabs, scratches, sores, and ulcers.
Eye involvement can lead to irritation, dryness, sensitivity to light, blurred vision, corneal scarring, and even blindness.
The intensity of itching is variable in linear IgA disease.
Linear IgA disease

Granuloma annulare
Linear IgA

Linear IgA

Linear IgA

String of beads sign

Chronic bullous disease of childhood.
What is the cause of linear IgA bullous disease?
The cause of linear IgA bullous disease is not fully understood. It is classified as an autoimmune skin disease. Blisters occur due to the development of a division between the epidermis and the dermiswhere IgA autoantibodies react to the components of the hemidesmosome and basement membrane (BP180, BP230, and LAD285).
Linear IgA bullous disease usually arises spontaneously, but can be triggered by a infection or medication.
Associations of underlying diseases
Linear IgA bullous dermatosis has been reported in patients with inflammatory gastrointestinal disease. It is thought that autoantigens they are exposed to the immune system in the diseased colon, and the autoantigens themselves target the skin. Surgery to remove the intestine can lead to the removal of the blistering disease of the skin.
Linear IgA bullous dermatosis has also been rarely associated with lymphoma, hematological conditions, rheumatic conditions and solid tumors
Drug-induced linear IgA bullous dermatosis.
Linear IgA dermatosis bullosa has been reported to be caused by medications. The most frequently associated drug is vancomycin. Other medications associated with linear IgA bullous dermatosis are:
- Diclofenac
- Captopril
- Trimethoprim + sulfamethoxazole
- Amiodarone
- Cyclosporine
- Glibenclamide
- Lithium
- Penicillin
- Cephamandol
- Phenytoin
- Somatostatin
- Sodium hypochlorite (bleach)
Drug-induced disease resolves with removal of the offending agent.
Linear IgA bullous disease presenting as toxic epidermal necrolysis
Toxic epidermal necrolysis (NET) is a serious disease. cutaneous adverse reaction to a drug that comes with extended Painful loss of skin and blisters. Some cases have been described in which direct immunofluorescence has revealed characteristic linear IgA deposits.
Worsening of linear IgA disease induced by TEN-type drugs *

Linear IgA

Linear IgA

Linear IgA
* The patient illustrated above developed a TEN-like eruption when dapsone is prescribed, it is normally beneficial in linear IgA disease.
What are the biopsy findings?
Linear IgA bullous dermatosis is a subepidermal bullous disorder. This means that a skin biopsy reports blisters just below the epidermis. It is associated with inflammation in which eosinophils and neutrophils are prominent
A special skin biopsy. antibody staining, direct immunofluorescence, reveals the immunoglobulin IgA along the basement membrane of the epidermis in a linear pattern. Sometimes these IgA antibodies can also be detected by a blood test (indirect immunofluorescence).
It is sometimes difficult to distinguish clinically different forms of immunobular diseases and histologically, and the antibody findings may overlap.
Direct immunofluorescence in linear IgA bullous dermatosis
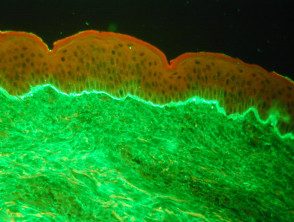
IgA linear deposition
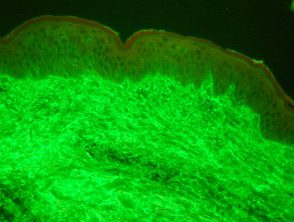
No IgG deposition
What is the treatment for linear IgA bullous dermatosis?
Most patients with linear IgA bullous dermatosis improve or disappear with dapsone 50–100 mg daily. Other medications that have been reported to help individual patients include:
-
Corticosteroids (prednisone or prednisolone)
-
Tetracycline antibiotics (not suitable in children younger than 8 years)
-
Erythromycin.
- Sulfapyridine
- Colchicine
- Mycophenolate mofetil
- Intravenous immunoglobulins
Although linear IgA bullous dermatosis may eventually disappear, many patients require long-term treatment, as a reduction in the dosage of the medication results in additional blisters.
